-

- Find a therapist
-
Find help
Life Challenges
Relationships
Trauma and Healing
Therapy Methods
Body and Mind
- Tests
- Blog

Eating Disorder Statistics 2023
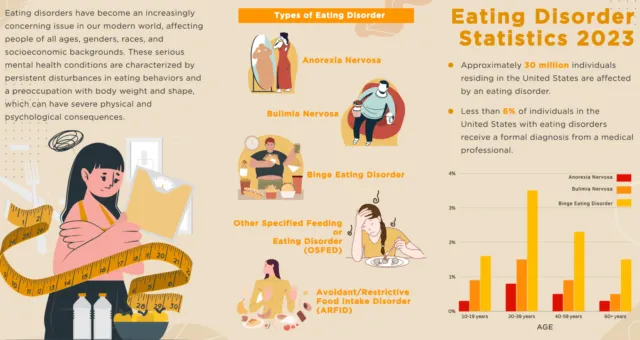
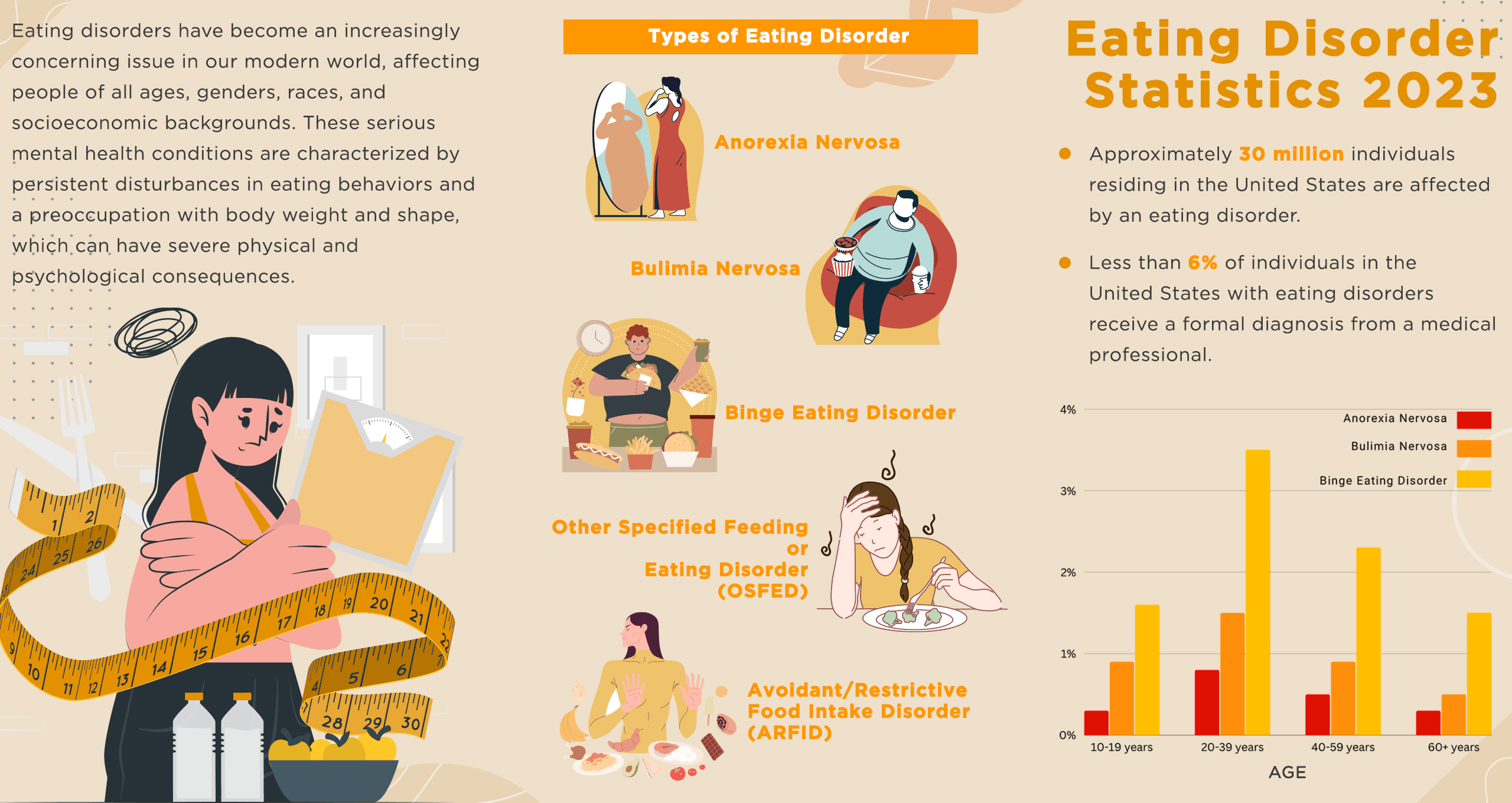
Eating disorders have become an increasingly concerning issue in our modern world, affecting people of all ages, genders, races, and socioeconomic backgrounds. These serious mental health conditions are characterized by persistent disturbances in eating behaviors and a preoccupation with body weight and shape, which can have severe physical and psychological consequences.
Within the realm of eating disorders, a global concern impacting countless individuals, it is essential to grasp the significance of statistics. According to the World Health Organization, in 2019 alone, approximately 14 million people worldwide grappled with an eating disorder. By delving into a comprehensive exploration of research, this analysis sheds light on various critical aspects. These include prevalence rates across diverse populations and regions, underlying factors contributing to their development, and the profound influence of comorbid mental and physical health conditions on the outcomes of eating disorders.
Eating Disorders: Understanding the Scope of Prevalence
According to a 2019 study, body dissatisfaction is prevalent among both men and women. Approximately 20% to 40% of women and 10% to 30% of men experience body dissatisfaction. Among male adolescents, a staggering 69% are dissatisfied with their weight. Social pressures and perceived stigma associated with being overweight or obese are the probable reasons for this phenomenon. Men are more likely to report overeating, while women are more likely to experience a sense of loss of control while eating.
Although gender differences were statistically significant, with women reporting higher levels of body checking, avoidance, binge eating, fasting, and vomiting, it is important to note that eating disorders affect both males and females equally. The myth that eating disorders are mostly prevalent in girls and women is untrue, and boys and men are just as susceptible to these conditions.
Understanding the Spectrum of Eating Disorders: Prevalence Rates and Types.
Anorexia Nervosa
Anorexia nervosa is a serious and potentially life-threatening eating disorder characterized by an intense fear of gaining weight, a distorted body image, and a severely restricted diet. It has the highest mortality rate of any psychiatric disorder. Research has suggested that anorexia nervosa has been on the rise since the 1950s, although changes in the diagnostic criteria for the disorder over time have made it difficult to compare prevalence rates directly.
In 2007, a study showed that anorexia nervosa was increasing by 36% every five years since the 1950s, affecting at least 8 million people globally. The most vulnerable age group for the disorder was found to be 15-24-year-old women due to societal pressures, genetics, and psychological factors.
More recent research conducted in 2021 indicates that the lifetime prevalence rates of anorexia nervosa among females may be as high as 4%, while males have a prevalence rate of 0.3%. Despite advancements in understanding and treating eating disorders, anorexia nervosa remains a serious and potentially life-threatening illness that requires prompt and effective treatment.
Gender differences in prevalence rates:
Anorexia nervosa is more common in females than in males, with an estimated female-to-male ratio of 10:1.
According to global data, the lifetime occurrence of anorexia nervosa is between 0.3% to 1.5% in females and 0.1% to 0.5% in males.
In a study in 2010, researchers found that females were significantly more likely than males to report disordered eating behaviors and attitudes.
According to researchers' findings from 2001 to 2004, globally the prevalence of anorexia nervosa in men is 0.3%, while women account for 0.9%.
Gender differences in risk factors:
Research has suggested that certain risk factors for anorexia nervosa may be more common in females than males, such as dieting behaviors and body dissatisfaction
In a study of 238 female and 85 male undergraduates at a Canadian university, researchers found that females were more likely than males to report unhealthy weight control behaviors and body dissatisfaction.
Researchers conducting a study on adolescent twins in 2009 found that anorexia nervosa genetic risk factors were more closely linked to the condition in females than in males.
Bulimia Nervosa
Bulimia nervosa is a serious eating disorder characterized by recurring episodes of binge eating followed by compensatory behaviors such as self-induced vomiting, misuse of laxatives or diuretics, or excessive exercise. This disorder often involves a distorted body image and a sense of loss of control over eating behavior.
First described in 1979 by British psychiatrist Gerald Russell as a chronic phase of anorexia nervosa, bulimia nervosa has seen a decline in incidence rates over time. The peak age of incidence ranges from 15 to 29 years, and while data on males with the disorder is scarce, rates are generally lower than those in females.
A recent review in the United States estimated the lifetime prevalence of bulimia nervosa to be 0.3% overall, with higher rates in females (0.5%) than in males (0.08%). While these numbers suggest a relatively stable prevalence of the disorder, it is important to note that many individuals with bulimia nervosa may not seek or receive treatment, and cultural factors may contribute to higher prevalence rates in certain populations.
Gender differences in prevalence rates:
According to researchers' findings from 2001 to 2004, globally the prevalence of Bulimia Nervosa in men is 0.5%, while women account for 1.5%.
Bulimia nervosa is estimated to affect 1-1.5% of females, with a 10:1 ratio of females to males suffering from the disorder, as reported by the American Psychiatric Association in 2013.
A study conducted in 2008 in Iceland among individuals aged 15-20 years found that bulimia nervosa was more prevalent in females than males. The study revealed that 5.6% of females and 0.8% of males were diagnosed with bulimia nervosa.
Based on data from 2001-2003, the prevalence of bulimia nervosa was significantly higher among females, with a rate of 0.5%, compared to males, who had a lower rate of 0.1%.
Based on information from the National Eating Disorders Association, research indicates that the prevalence of bulimia nervosa varies among different populations. It is estimated that between 1.1% and 4.6% of females and 0.1% to 0.5% of males will develop bulimia nervosa at some point in their lives.
Gender differences in risk factors:
Research has suggested that certain risk factors for bulimia nervosa may be more common in females than males, such as body dissatisfaction and emotional dysregulation.
In the study, researchers found that females were more likely than males to report body dissatisfaction and negative affect, which were significant predictors of bulimic symptoms.
In a study conducted with patients diagnosed with eating disorders in Spain, researchers observed that emotional dysregulation played a significant role in predicting bulimic symptoms, particularly among females. However, the impact of emotional dysregulation on bulimic symptoms was not found to be significant among males. This highlights the gender-specific nature of the association between emotional dysregulation and bulimic behaviors in the Spanish sample.
Binge Eating Disorder
Binge Eating Disorder (BED) is a serious eating disorder characterized by recurring episodes of eating large amounts of food in a short period of time while experiencing a sense of loss of control. Unlike bulimia nervosa, individuals with BED do not engage in compensatory behaviors such as self-induced vomiting or excessive exercise.
First recognized in a 1959 paper by psychiatrist Albert Stunkard, BED was only officially included as a distinct eating disorder in the DSM-5, published in 2013. As a result, historical prevalence rates for BED are unknown. However, recent research suggests that the disorder's prevalence has been increasing over time.
Lifetime prevalence estimates for BED-broad are 0.74% for males and 1.85% for females, which is higher than previous research had indicated. A more recent study in January 2020 found current prevalence rates (past 3 months) of 0.03% for males and 0.20% for females.
The estimated lifetime prevalence of BED in the US, based on DSM-IV criteria, is 1.9%-2.8%. Despite this growing awareness of BED as a distinct disorder, underdiagnosis and undertreatment remain a significant concern, highlighting the need for greater education and resources in the prevention, identification, and treatment of BED.
Gender differences in prevalence rates:
A recent study stated that the point prevalence of binge eating disorder (BED) in children worldwide is 0.7%, while the one-year point prevalence of BED in adults is 1.1%, and the lifetime prevalence of BED in adults is 2.3%.
Researchers estimate that 60% of individuals with BED are women.
Binge Eating Disorder (BED) is the most common eating disorder in males, affecting 36% of men and boys. Among individuals diagnosed with BED, 40% are male.
According to a study conducted in the United States, the lifetime prevalence of binge eating disorder (BED) was found to be 3.5% among females and 2% among males. This indicates that BED is more prevalent than anorexia and bulimia combined, and even more so than breast cancer, HIV, and schizophrenia.
Research indicates that projections for 2030 suggest that around half a million men in the United States will experience binge eating disorder (BED), while approximately 1.5 million women will be affected by BED.
The one-year prevalence of binge eating disorder (BED) in men is 0.26%, and among men aged 10-19 years, the prevalence is even higher at 0.48%. Conversely, women aged 20-29 years have the highest estimated BED prevalence rates, reaching 2.09%.
Gender differences in risk factors:
Research has suggested that certain risk factors for binge eating disorder may be more common in females than males, such as body dissatisfaction, weight-related concerns, and negative affect..
A study in 2019 found that females were more likely than males to report body dissatisfaction and depressive symptoms, which were both significant predictors of binge eating behavior (Eating Behaviors).
In a study of adolescents, researchers found that weight-related teasing and internalization of the thin ideal were stronger predictors of binge eating in females than in males (International Journal of Eating Disorders).
Other Specified Feeding or Eating Disorder (OSFED)
Other Specified Feeding or Eating Disorder (OSFED) is a category of eating disorders that includes a range of disordered eating behaviors that do not meet the diagnostic criteria for anorexia nervosa, bulimia nervosa, or binge eating disorder. Although OSFED may include behaviors such as recurrent episodes of binge eating, purging, or restrictive eating, the frequency, duration, or intensity of these behaviors may not meet the diagnostic criteria for other eating disorders.
The DSM-5 added OSFED in 2013 to replace the previous category of Eating Disorder Not Otherwise Specified (EDNOS). The change in diagnostic criteria and terminology has made it challenging to compare prevalence rates over time. However, recent studies indicate that other specified feeding or eating disorders (OSFED) have surpassed other eating disorder categories to become the most prevalent diagnosis, accounting for approximately 70% of all cases.
Few studies have examined the prevalence of OSFED. In the largest community study to date, 496 adolescent females completed annual diagnostic interviews over eight years. By age 20, lifetime prevalence for OSFED overall was 11.5%, with the peak age of onset being 18-20 years.
Gender differences in prevalence rates:
Additional research is imperative to comprehensively comprehend the gender disparities in OSFED, as the current literature on this specific domain remains relatively constrained. However, the existing statistics we have collected provide valuable insights:
According to a recent study conducted in March 2023, it was found that Other Specified Feeding or Eating Disorder (OSFED) is the prevailing eating disorder in the United States, affecting approximately 1.18% of American women.
A 2020 study disclosed that, similar to the one-year prevalence rates, other specified feeding or eating disorders (OSFED) emerged as the most prevalent eating disorder experienced throughout an individual's lifetime. Among females, the prevalence of OSFED was found to be 3.82%, while among males it was 1.61%.
In a 2017 examination of eating disorders among a sample of 342 elderly women aged 65-94 in the Azores (Portugal), it was discovered that the most prevalent eating disorder among this group was other specified feeding and eating disorders (OSFED) with a prevalence rate of 1.5%.
In a recently published two-stage study involving a large sample of 5658 midlife women from the United Kingdom, the lifetime and 12-month prevalence of eating disorders were examined. Among the 40-50-year-old women, the 12-month prevalence of eating disorders was found to be 3.6%
Another study with a total of 797 participants (50.8% females) were assessed for eating disorder risk/diagnostic category. The point prevalence of OSFED was observed as 5.7% for OSFED-BN (5.7% males; 5.8% females) and 30.9% for OSFED-other (34.9% males; 27.0% females).
In a study of individuals seeking treatment for eating disorders, researchers found that males with OSFED were more likely to present with muscle dysmorphia, whereas females were more likely to exhibit atypical anorexia nervosa or purging disorder (International Journal of Eating Disorders).
Among the various types of eating disorders, other specified feeding or eating disorders (OSFED) accounted for a prevalence rate of 0.6%. Remarkably, OSFED emerged as the most prevalent eating disorder category, surpassing other subtypes. Notably, the most commonly reported symptom associated with OSFED was "body image disturbance," underscoring its prominence and impact within this disorder.
Avoidant/Restrictive Food Intake Disorder (ARFID)
Avoidant/Restrictive Food Intake Disorder (ARFID) is a newer category of eating disorder that is characterized by a persistent disturbance in eating or feeding, leading to an insufficient intake of nutrients or calories. Unlike other eating disorders, ARFID is not driven by concerns about weight or body shape, but instead by factors such as sensory sensitivity, fear of vomiting or choking, or lack of interest in food.
ARFID was added to the DSM-5 in 2013 to replace the previous diagnosis of Feeding Disorder in Infancy or Early Childhood, making it challenging to compare prevalence rates over time. However, recent studies suggest that ARFID may be more common than previously recognized, particularly among children and adolescents.
Research from non-clinical samples has reported ARFID prevalence estimates ranging from 0.3% to 15.5%. One study, which used national surveillance methodology, found that the incidence of ARFID in children and adolescents who received clinical care was 2.02 per 100,000 patients.
Gender differences in prevalence rates:
Research on gender differences in Avoidant/Restrictive Food Intake Disorder (ARFID) is limited, and there is a scarcity of specific statistics on gender prevalence rates. However, here are some insights based on available information:
Recent studies indicate that individuals with Avoidant/Restrictive Food Intake Disorder (ARFID) tend to be younger when seeking treatment compared to other eating disorders. Moreover, research suggests that ARFID may have a higher prevalence among males, particularly in pediatric treatment settings.
Several studies conducted in 2021 have consistently found a higher prevalence of male patients in the diagnosis of Avoidant/Restrictive Food Intake Disorder (ARFID) when compared to other eating disorder groups.
In 2021, a study involving a total of 61 participants revealed that among the participants, there were 27 males, 28 females, and 6 transgender youths. The findings of the study indicated that 9 of the males, 8 of the females, and 1 of the transgender individuals met the criteria for Avoidant/Restrictive Food Intake Disorder (ARFID).
Breaking Down the Numbers: Eating Disorder Prevalence Rates Across Demographics
Global prevalence rates of eating disorders:
The global prevalence of eating disorders has been increasing over the years, with recent statistics revealing that approximately 70 million individuals across the world are currently living with eating disorders. Studies indicate that the global prevalence of eating disorders has increased from 3.4% to 7.8% between 2000 and 2018. In 2022, eating disorders affect at least 9% of the global population. Current research shows that the global lifetime prevalence of any eating disorder ranges from 0.74 to 2.2% in males, and 2.58–8.4% in females.
Top Countries with the Highest Eating Disorder Rates
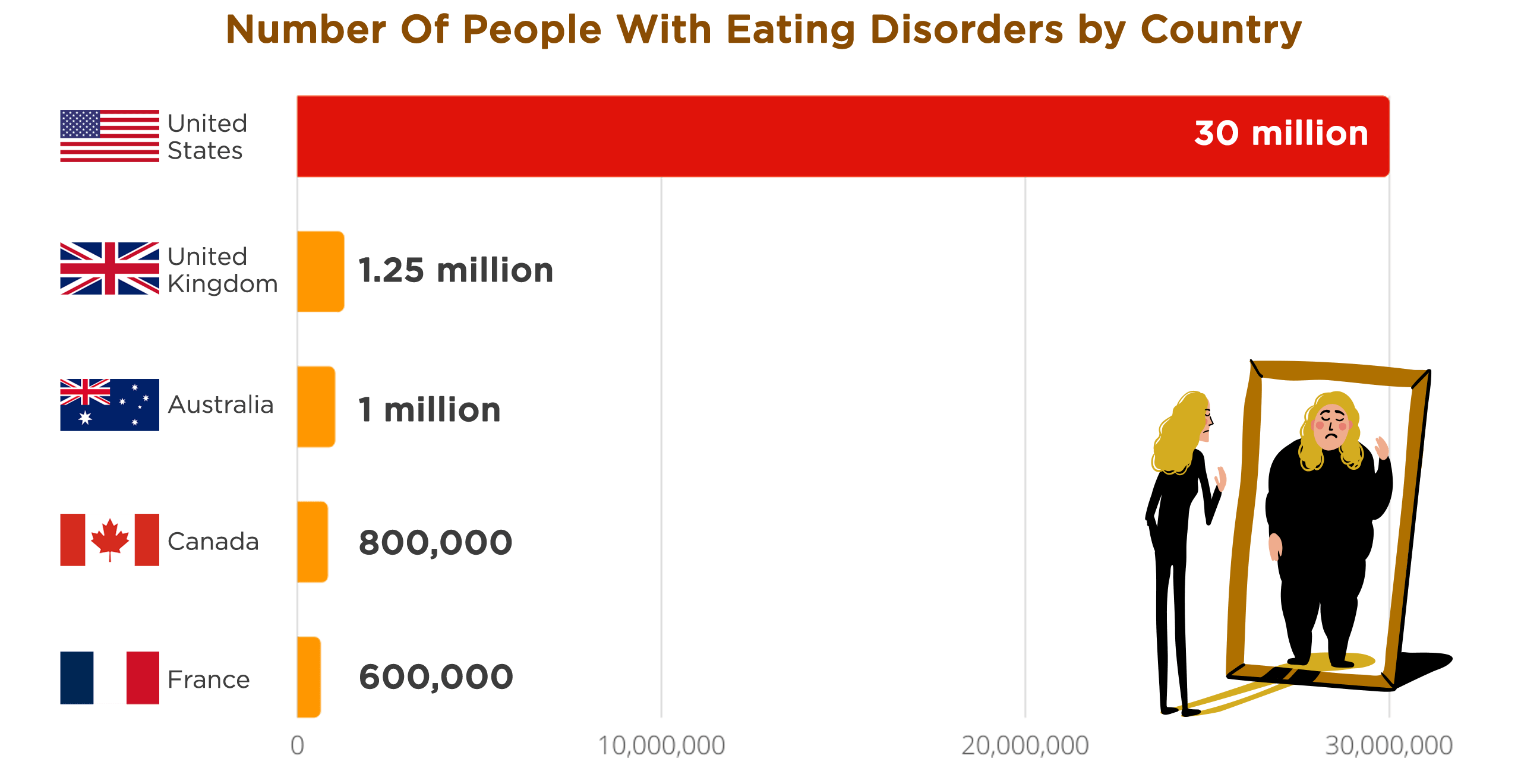
As of 2022, there are approximately 30 million individuals in the United States who are living with an eating disorder. Moreover, another study conducted in 2022 revealed that 9% of the U.S. population is currently affected by eating disorders.
According to The National Eating Disorder Centre (NEDIC) in Canada, between 840,000 and 1,750,000 people in the country have symptoms of eating disorders at any given time. This estimate was made in 2022.
According to the Butterfly Foundation, over 1 million Australians are living with an eating disorder.
In the United Kingdom, between 1.25 and 3.4 million individuals are affected by an eating disorder. Approximately 25% of those affected are male.
Spain recorded more than 79,000 cases of anorexia nervosa or bulimia in 2020, an increase from the 77,500 cases reported the previous year. Compared to 2011, when there were 14,600 cases of anorexia nervosa or bulimia, the number of eating disorder cases in the country has increased by over 400 percent.
According to a 2017 study, eating disorders affect approximately 600,000 young people in France, with 40,000 of those individuals experiencing anorexia. The majority of those affected are women. Analysis from 2009 found that France has a lifetime prevalence of eating disorders of 4.15%, according to a study with a confidence interval of 2.3-7.4.
Based on a study published in the "Journal of Psychiatric Research," Italy has an estimated prevalence rate of around 3.35% for eating disorders. As of 2021, it is believed that approximately 3 million people in Italy are affected by eating disorders.
In Germany, prevalence estimates for eating disorders vary depending on the threshold. For any threshold eating disorder, estimates range from 2.9% in females to 0.1% in males. For any subthreshold eating disorder, estimates range from 2.2% in females to 0.7% in males. Eating disorder symptoms are reported by 11.5% of females and 1.8% of males.
In Brazil, around 0.4% of children between the ages of 6 and 14 have been identified as having an eating disorder. Additionally, the point-prevalence of bulimia nervosa is 0.7%, binge-eating disorder is 1.4%, and recurrent binge eating is 6.2%. These statistics are based on studies with confidence intervals ranging from 0.34 to 5.27.
Japan has emerged as having the highest prevalence of eating disorders in Asia, with Hong Kong, Singapore, Taiwan, and South Korea following closely behind. In 2017, data from "Our World in Data" showed that 397,994 people of any age in Japan had been diagnosed with an eating disorder. While the prevalence of eating disorders in Japan is 0.33% for individuals of all ages, it is particularly high among those between 20-24 years old, with a prevalence of 1.03% in 2017.
Regional prevalence rates of eating disorders:
Asia - Japan, followed by Hong Kong, Singapore, Taiwan, and South Korea, has the highest prevalence of eating disorders. Additionally, the Philippines, Malaysia, Indonesia, Thailand, China, and Vietnam have also experienced an increase in eating disorders as industrialization and globalization progress, leading to growing concerns about body shape and size.
In Hong Kong, a study revealed that out of 857 adolescent female students who desired to lose weight, only 4.8% were actually overweight, suggesting the influence of social pressures, mental health issues, and the local environment and culture on eating problems and disorders. Another study examining eating disorders between 1987 and 2007 found that the majority of affected individuals were single females in their 20s. The study included 195 patients, with 59% diagnosed with anorexia nervosa and 40% with bulimia nervosa. These findings align with global trends in eating disorders.
In Singapore, eating disorders, particularly body dissatisfaction, have become more prevalent since the 1990s. A 2003 study examining eating disorder development by ethnicity reported that 91.3% of cases were female, while 8.7% were male. Between 1994 and 2002, two eating disorder clinics in Singapore treated a total of 126 individuals with anorexia nervosa (AN), and during that period, the number of new AN cases per year quadrupled. In 2017, the number of Singaporeans with an eating disorder, across all age groups, was 30,956.
A recent study in Taiwan examined the prevalence of eating disorders from 2002 to 2013. It found that during this period, there were a total of 1,893 cases of anorexia nervosa (AN) and 10,542 cases of bulimia nervosa (BN). The overall incidence rates of AN and BN in Taiwan were 1.1 and 6.1 per 100,000 people, respectively. Most individuals with AN and BN were in the 20-29 age range. The study also revealed an increase in the overall incidence of AN and BN during the study period, from 0.96 to 1.27 per 100,000 people.
The influence of K-pop culture on promoting extremely thin body shape and the rise of the Mukbang internet phenomenon have raised concerns about the development of eating disorders in South Korea. An early study reported that 8.5% of South Koreans exhibited abnormal eating pathology. The lifetime prevalence of anorexia nervosa (AN) and bulimia nervosa (BN) among Koreans is 0.01% and 0.1% respectively. In 2011, there were 159 reported cases of eating disorders among South Koreans aged 19-30, but by 2017, the number of individuals with eating disorders of any age in South Korea had risen to 189,698.
Europe - As of 2012, Austria stood out with the highest prevalence rate of eating disorders in Europe, reaching 1.55%. When examining the overall impact, it is estimated that approximately 20 million individuals in Europe are affected by eating disorders in 2021. To provide further insight into this matter, we present below the key findings from a comprehensive narrative review of European studies on eating disorders published between 2015 and the first half of 2016.
Prevalence:
Anorexia nervosa: Reported by 1-4% of women in Europe.
Bulimia nervosa: Reported by 1-2% of women in Europe.
Binge eating disorder: Reported by 1-4% of women in Europe.
Subthreshold eating disorders: Reported by 2-3% of women in Europe.
Men: 0.3-0.7% report eating disorders.
Comorbidity:
Over 70% of individuals with eating disorders report comorbid disorders.
Common comorbid disorders include anxiety disorders 50%, mood disorders 40%, self-harm 20%, and substance use 10%.
The Journal of Psychiatric Research published a study in 2009 that examined the lifetime prevalence estimates of Eating Disorders in several European countries. Here are the key findings:
Lifetime prevalence estimates of eating disorders varied across different countries:
France: 4.15%
Belgium: 3.54%
Italy: 3.35%
Netherlands: 1.74%
Germany: 1.28%
Spain: 2.42%
Germany and the Netherlands had the lowest estimates of lifetime prevalence for anorexia nervosa. Germany and Italy had the lowest estimates of lifetime prevalence for bulimia nervosa.
The ESEMeD project, conducted between January 2001 and August 2003, aimed to examine the prevalence of non-psychotic mental disorders in six European countries: Belgium, France, Germany, Italy, the Netherlands, and Spain. A total of 21,425 respondents aged 18 or older participated in the study. Within this larger sample, a subsample of 4,139 respondents underwent a detailed investigation specifically focused on Eating Disorders.
The estimated lifetime prevalence rates of different Eating Disorders were as follows:
Anorexia nervosa: 0.48%
Bulimia nervosa: 0.51%
Binge eating disorder: 1.12%
Subthreshold binge eating disorder: 0.72%
Any binge eating: 2.15%
These prevalence rates were consistently 3-8 times higher among women compared to men for all types of Eating Disorders.
Latin America - In 2016, an analysis was conducted to examine the prevalence of eating disorders in Latin America compared to Western countries. The findings suggest that bulimia nervosa and binge eating disorder appear to be more prevalent in Latin America. The analysis included 17 studies from Argentina, Brazil, Chile, Colombia, Mexico, and Venezuela, out of a total of 1,583 records screened. These studies revealed that the mean point-prevalence rate of anorexia nervosa was 0.1%, bulimia nervosa was 1.16%, and binge-eating disorder was 3.53% in the general population.
Here are additional key statistics derived from the same analysis:
Mexico (Adolescents aged 12-17 years):
Anorexia nervosa:
Lifetime prevalence: 0.5%
12-month prevalence: 0.1%
Bulimia nervosa:
Lifetime prevalence: 1.0%
12-month prevalence: 0.7%
Binge Eating Disorder:
Lifetime prevalence: 1.4%
12-month prevalence: 0.7%
Mexico (Adults):
Bulimia nervosa:
Lifetime prevalence: 0.8%
12-month prevalence: 0.3%
Colombia (Adults):
Bulimia nervosa:
Lifetime prevalence: 0.4%
12-month prevalence: 0.2%
Brazil (Adults):
Bulimia nervosa:
Lifetime prevalence: 2.0%
12-month prevalence: 0.9%
Binge Eating Disorder:
Lifetime prevalence: 4.7%
12-month prevalence: 1.8%
It is worth noting that lifetime prevalence rates were highest for bulimia nervosa and Binge Eating Disorder in Brazil, and lowest in Colombia.
In 2011, studies conducted using Latin American samples identified individuals who met partial or complete DSM-IV diagnostic criteria for binge eating disorder, revealing that this disorder is indeed present in Latin America and shares clinical features similar to those observed in the international literature. Among obese individuals participating in weight loss programs, the prevalence of binge eating disorder ranged from 16% to 51.6%. When comparing obese individuals with and without binge eating disorder, several trends were observed. Those with binge eating disorder tended to have higher weight, a longer history of weight fluctuation, increased concern about shape and weight, and a higher likelihood of psychiatric comorbidity.
MENA Region (Middle East and North Africa) - In the MENA region, the prevalence of Anorexia nervosa has escalated between 1990 and 2019, indicating a heightened burden on public health. With the growing population and swift fluctuations in the frequency of various prominent risk factors, Anorexia nervosa is poised to evolve into a more pressing public health concern in the foreseeable future. Here are some significant statistics derived from an analysis published in 2022:
The age-standardized prevalence rate of eating disorders in the MENA Region in 2019 was 216.9 individuals per 100,000 population, higher than the global average of 174.0 cases per 100,000.
The prevalence of Anorexia nervosa in the MENA region, according to GBD 2017 data, was lower than the global average (32.8 vs. 43.8 per 100,000 population, respectively).
The annual increase in the disability-adjusted life-years rate attributed to Anorexia nervosa over the past 30 years was higher in MENA (0.69) compared to the global average (0.45).
In Iran, a study estimated that the prevalence rate of Anorexia nervosa was 9.42 times higher in females than in males and 6.02 times higher in older adolescents compared to early childhood.
A study conducted in Turkey among nursing students found an estimated prevalence rate of Anorexia nervosa to be 0.5%.
The higher rate found in the Turkish study can be attributed to its focus on female college students aged between 16 and 24 years, limiting its generalizability to the general population.
Middle East - In 2022, researchers conducted a comprehensive survey of 49 studies examining the prevalence of disordered eating attitudes and Eating Disorders in Arab countries. The sample included 12 out of the 22 member countries in the League of Arab States, with a total of 17,679 students aged 12-33. The findings revealed the following:
The average prevalence of disordered eating attitudes and Eating Disorders across the 12 included member countries was 31.4%.
Significant variations in prevalence were observed between the countries.
Egypt and Lebanon had the highest prevalence rates, with 73.3% and 74.5% respectively, but these rates were based on only one study in each country.
Morocco had the lowest reported prevalence rate at 9.6%, although this study only assessed bulimia nervosa and did not include other Eating Disorders.
In the Kingdom of Saudi Arabia, the average prevalence across studies was 29.7%, ranging from 21% in Ha'il to 45.5% in Dammam.
Sudan, Jordan, and the UAE had lower average prevalence rates compared to the Kingdom of Saudi Arabia, at 21.1%, 18.9%, and 20% respectively.
Kuwait had a higher average prevalence rate of 46.4% compared to the Kingdom of Saudi Arabia.
Another review undertaken in 2019 explored the prevalence of disordered eating attitudes and Eating Disorders in Arab countries, offering valuable insights into the issue.
The overall estimated prevalence of disordered eating attitudes among Arab adolescents was 26.94%.
This indicates a higher prevalence of abnormal eating attitudes among Arabs compared to the adolescent population in the USA and sub-Saharan Africa.
Prevalence varied across countries, with rates ranging from 11.5% (Egypt) to 49.1% (UAE) in females and from 6% (Saudi Arabia) to 36.4% (Oman) in males.
The highest prevalence of disordered eating attitudes was reported in UAE and Saudi Arabian adolescents.
Africa - In a comprehensive review conducted in 2020, the prevalence of different eating disorder subtypes among patients diagnosed at a South African tertiary hospital over a span of 21 years was analyzed. The findings revealed that 40.1% of the diagnosed cases were classified as bulimia nervosa, 33.3% as eating disorders not otherwise specified, and 26.5% as anorexia nervosa. Furthermore, a significant majority of the participants (71.0%) reported the use of at least one substance, with alcohol being the most commonly reported substance of choice (54.8%).
In a study conducted in West Africa, the researchers examined the prevalence of eating disorders and factors that contribute to their development among 696 female adolescents aged 12-20 years. The findings revealed that 16% of the respondents had a body mass index (BMI) below the 5th percentile, as per the World Health Organization age-standardized criteria, while 4% were above the 85th percentile. Interestingly, most of the respondents expressed a desire to have a larger body size.
In terms of specific eating disorders, four out of the 696 respondents (0.6%) met the DSM-5 criteria for anorexia nervosa, none met the criteria for bulimia nervosa, and two (0.3%) fulfilled the criteria for binge eating disorder. It is worth noting that the point prevalence of BN in young African women has been estimated to be 0.87%, which falls within the range reported for young women in high-income countries and Latin America.
In 2016, a comprehensive review of four studies on the epidemiology of eating disorders in Africa yielded important and formally assessed data on specific eating disorders. Among a total of 1476 young females included in these studies, no cases of anorexia nervosa, as defined by the Diagnostic and Statistical Manual of Mental Disorders-IV criteria, were found.
However, the combined point-prevalence rate of bulimia nervosa among young women in Africa was estimated to be 0.87%, indicating the presence of this eating disorder in the population. Additionally, the combined point-prevalence rate of eating disorders not otherwise specified was estimated to be 4.45% among young women in Africa.
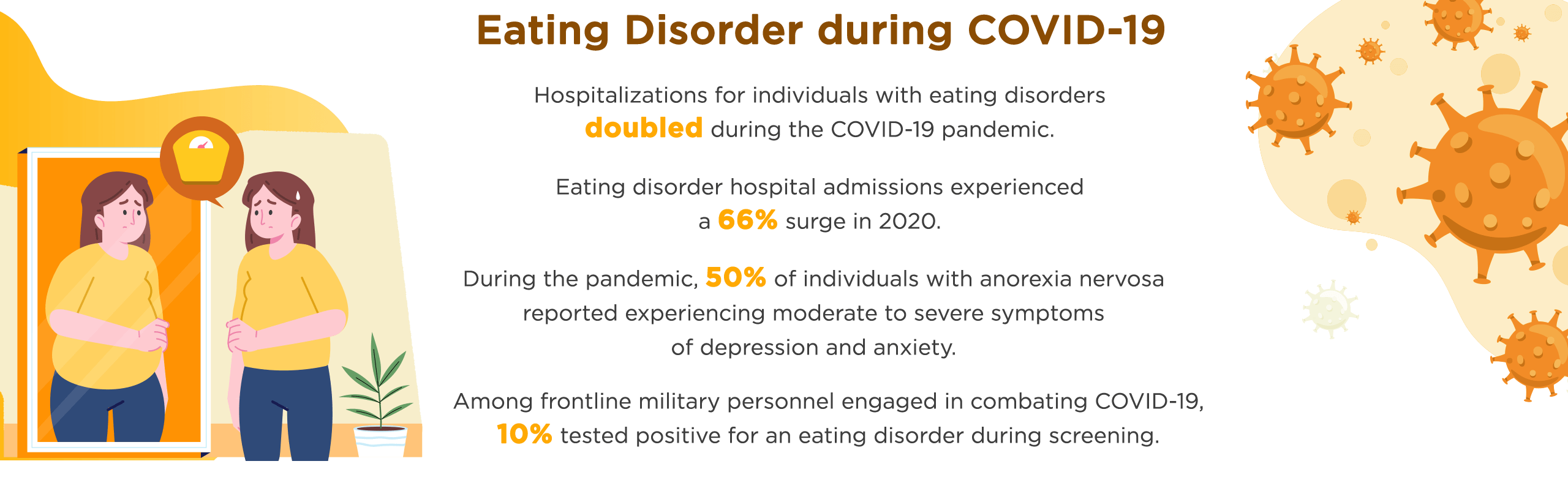
Eating disorders during COVID-19
The COVID-19 pandemic has had a profound impact on individuals worldwide, including an alarming increase in eating disorders and related behaviors. Let's explore the most recent statistics from recent research studies conducted during this period to better understand the impact of COVID-19 on eating disorders.
During the pandemic:
65% of individuals with an eating disorder reported an increase in food restriction.
35% of individuals with an eating disorder reported more frequent episodes of binge eating.
19% of individuals with an eating disorder reported more frequent episodes of purging.
Specifically, among individuals with anorexia nervosa:
50% experienced moderate to severe symptoms of depression and anxiety.
In German women with anorexia nervosa, 40% stated that their symptoms worsened, 20% developed new symptoms, and 50% reported a significant impact on their quality of life.
Approximately 70% of the same sample of German women reported that their fear of weight gain, concerns with shape, weight, and eating, and drive for thinness worsened during the pandemic.
In the general population:
27% of Australians reported more severe food restrictions.
34% of Australians reported increased episodes of binge eating.
In a sample of UK women with eating disorders:
80% reported that their symptoms worsened during the lockdown.
2022 data obtained from PubMed, Scopus, and Cochrane Library in 2022 shed light on the impact of the COVID-19 pandemic on eating disorders, revealing concerning trends:
In England, the impact of the COVID-19 pandemic on eating disorders has been substantial, as indicated by the following statistics: Following the COVID-19 lockdown, there was a significant increase in eating disorder symptomatology scores, suggesting a worsening of symptoms among affected individuals.
A staggering 86.7% of individuals with eating disorders in England reported that their symptoms had worsened during the pandemic lockdown. Among them, 30% believed that their symptoms had significantly deteriorated, highlighting the severity of the situation. Furthermore, participants from England described the lockdown as detrimental to their well-being, with 36% experiencing changes in their eating behaviors. Notably, 3867 individuals reported persistently eating more throughout the lockdown period.
In Spain, a substantial 41.9% of participants reported a reactivation of eating disorder (ED) symptoms. The exacerbation of symptoms was primarily attributed to food restriction and social isolation, highlighting the challenging circumstances faced by individuals.
Within the Spanish sample, approximately 25% of patients experienced a deterioration in their ED symptoms during the lockdown period. Notably, individuals with Anorexia Nervosa were particularly susceptible to a greater decline in symptomatology.
In Portugal, 31% of participants reported weight gain attributed to the COVID-19 lockdown. Those who experienced notable disruptions in their daily routines were more likely to develop symptoms of disordered eating and face clinical impairment.
Exploring the Influential Factors of Eating Disorder Prevalence Rates
Cultural and religious factors
Cultural norms and values related to body image and weight:
Research has shown that the Western ideal of thinness has become increasingly pervasive in non-Western cultures, contributing to the development of eating disorders
A study conducted by Becker discovered that individuals exposed to television had a significantly higher prevalence of disordered eating behaviors. The Fiji studies, which are often cited as compelling evidence, indicate that exposure to thin images in the mass media is associated with eating disorders. These findings have implications for American teen girls as well. It is noteworthy that 29.2% of participants scored high on the eating disorder behavior test administered by Becker.
Religious and cultural practices related to food and eating:
Religious and cultural practices related to food and eating can impact the development and management of eating disorders.
A study by a Registered Dietitian in 2022 showed that fasting during Ramadan can increase the risk of disordered eating behaviors. In the Arab world, individuals at high risk for eating disorders range from 2% to 54.8%, according to a literature review. Fasting can trigger a relapse and worsen eating disorders. Some individuals may use fasting to hide their disorder and continue their unhealthy eating habits. This is especially difficult for those who use religious devotion as a justification for their behavior. It can impede progress made during treatment and raise the risk of relapse.
Socioeconomic factors
Income and education:
Limited studies in 2017 have suggested a higher risk of eating disorders (EDs) among individuals with lower household incomes, yet these findings are constrained by small sample sizes that may not reflect the broader population accurately.
Another study was conducted on a population-based sample in Australia, regressions were performed to assess the likelihood of reporting eating disorder (ED) features among different income levels, compared to individuals with an income below $30,000 per year. The findings revealed that none of the measured ED features showed a significant association with household income.
A study conducted in 2021 revealed a significant association between lower education levels and an elevated risk of Binge Eating Disorder among Latinos residing in the United States.
Access to healthcare:
Individuals with higher socioeconomic backgrounds tend to have better access to resources and treatment options, resulting in higher rates of diagnosis and active pursuit of treatment for eating disorders. Conversely, research has revealed that individuals from lower socioeconomic backgrounds encounter obstacles that hinder their access to appropriate care, leading to underdiagnosis and inadequate treatment of eating disorders in these populations.
Disparities in access to care for eating disorders can be impacted by regional and socioeconomic factors.
A recent study revealed that access to eating disorder treatment is limited, particularly for children and adolescents with public insurance. The research found that individuals with public insurance are one-third less likely to receive proper treatment for eating disorders than those with private insurance. The study demonstrated that public insurance holders have significantly lower odds of receiving appropriate treatment for eating disorders.
Social factors
Social pressure and media influence:
Research suggests that exposure to idealized body images in the media can increase body dissatisfaction and contribute to disordered eating behaviors
Researchers have theorized that the media has a significant influence in the development and escalation of body dissatisfaction, which, in turn, may contribute to the rising prevalence of eating disorders. Specifically, in 2003, the rate of anorexia nervosa among girls aged 15 to 19 years was found to be 0.48%. Moreover, it is estimated that approximately 1% to 5% of adolescent girls meet the diagnostic criteria for bulimia nervosa.
The findings of a 2020 study revealed that 52% of girls and 45% of boys who participated reported engaging in behaviors related to eating disorders, including skipping meals. Although the study did not explicitly attribute eating disorders to social media, it emphasized the need to recognize and monitor the connection between social media and these disorders.
A study highlighted a significant transformation in the portrayal of female and male models in Western media and the prevailing notion of the "perfect" or "ideal" body. The cultural ideal for women's body size and shape has progressively shifted towards a thinner and leaner appearance. The findings indicated a substantial decrease in the body weights and measurements of the models, with 70% of women being underweight and over 75% falling below 85% of their ideal body weight.
Social comparison and peer influence:
Social comparison and peer influence play a significant role in the development of eating disorders.
Comparing oneself to others and perceiving pressure to conform to certain appearance ideals can contribute to body dissatisfaction and disordered eating.
The findings of a 2016 study revealed that the concept of "Pressure to be thin" encompasses sociocultural messages that promote the "thin ideal," which is a cultural perception of beauty centered around an extremely slim or lean body shape. This pressure is primarily propagated by Western media but can also be transmitted by parents and peers. It includes both positive reinforcement of thinness, such as complimenting thinness or weight loss, as well as negative behaviors like overt criticism or teasing about weight. Approximately 16-30% of teenagers reported experiencing pressure to be thin in various forms.
Race and Ethnicity Differences in Eating Disorder Prevalence Rates:
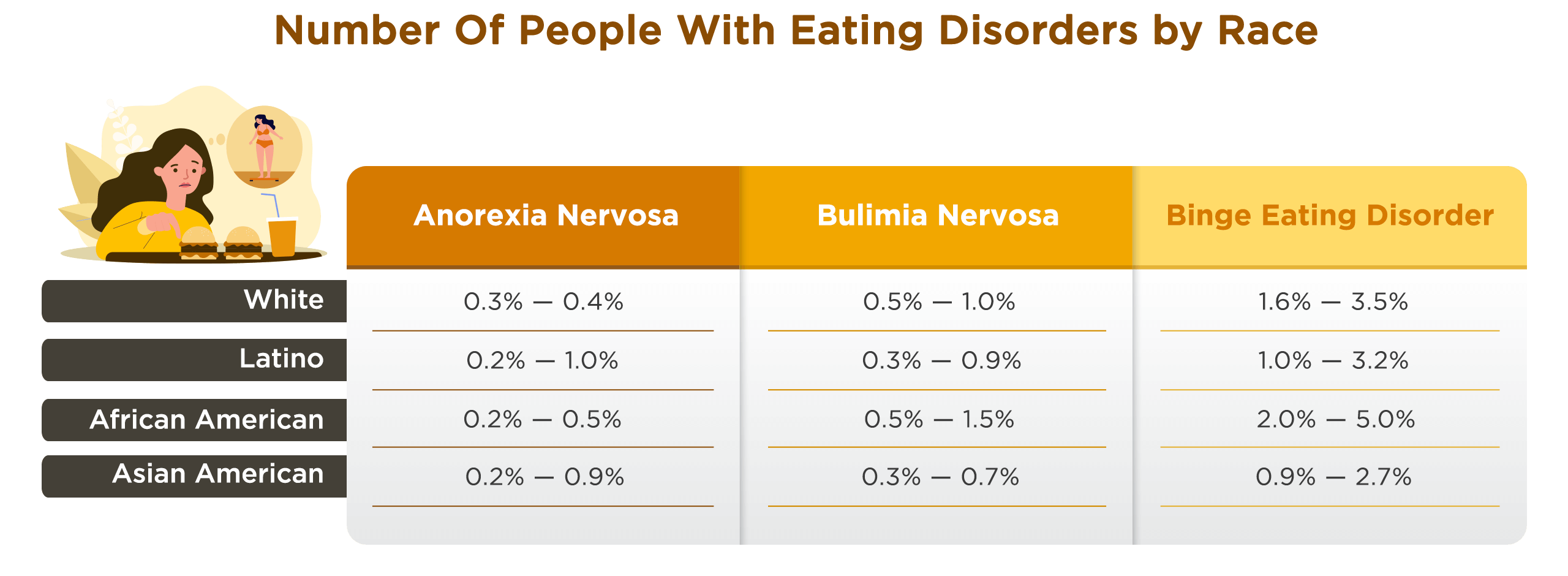
Prevalence rates among different racial and ethnic groups:
Research suggests that there are variations in eating disorder prevalence rates among different racial and ethnic groups.
An analysis of eating disorder symptoms among college students in the United States revealed that Latino/a students had higher rates of eating disorder symptoms compared to African-American, Asian, and white students.
During the year 2019, a study revealed that Asian American women had higher prevalence rates of eating disorders when compared to women from other ethnic backgrounds. Interestingly, their rates were found to be similar to those observed among European American women.
Disparities in diagnosis and treatment-seeking:
In a recent study, it was found that race/ethnicity played a significant role in the treatment outcomes of youth. Specifically, Latinx individuals were more likely to receive no treatment (21.3%) compared to Whites (11.4%)..
Factors such as lack of awareness, stigma, and limited access to culturally competent care may contribute to these disparities.
The findings of a 2019 study highlight the presence of ethnic/racial disparities in help-seeking behaviors for eating disorders. Specifically, the study reveals that individuals from ethnic/racial minority backgrounds were significantly less inclined to seek help compared to non-Hispanic white individuals, depending on the specific type of eating disorder.
Sexual orientation and eating disorder prevalence rates
Higher prevalence rates among sexual minority individuals:
In 2020, research has shown that eating disorders and disordered eating behaviors are more prevalent among LGBT individuals compared to heterosexual and cisgender individuals. The statistics highlight the extent of this issue:
Approximately 54% of LGBT adolescents have been diagnosed with a full-syndrome eating disorder in their lifetime.
An additional 21% of LGBT adolescents suspect they have experienced an eating disorder at some point in their lives.
In one study, 60.9% of LGBT adolescents reported engaging in at least one disordered eating behavior within the past year.
Another study reported that transgender youth had higher rates of eating disorders compared to cisgender youth.
According to data from the National College Health Assessment survey conducted by the American College Health Association between fall 2015 and spring 2019, the prevalence of eating disorders among college students is as follows:
Prevalence of Eating Disorders:
7.15% of the 414,299 students surveyed reported experiencing an eating disorder or receiving an eating disorder diagnosis.
Eating disorders were most prevalent among younger college students, with a prevalence of 7.95% among respondents aged 18-20.
Eating Disorders by Gender Identity and Sexual Orientation:
Transgender students had a prevalence of 17.50%.
Gender diverse students had a prevalence of 15.74%.
Cisgender female students had a prevalence of 8.12%.
Cisgender male students had a prevalence of 4.07%.
Sexual minority students had higher prevalence rates: gay/lesbian (10.18%), bisexual (14.03%), unsure/other (12.45%).
Factors Associated with Eating Disorders:
Students experiencing social relationship problems had a prevalence of 12.73%.
Students experiencing family problems had a prevalence of 11.62%.
Body image dissatisfaction and minority stress:
Sexual minority individuals may experience higher levels of body dissatisfaction due to minority stress, which includes experiences of discrimination, stigma, and prejudice.
Studies have indicated a clear correlation between minority stress and both binge eating behaviors and body dissatisfaction among lesbian and bisexual women. The impact of minority stress on these aspects of their well-being is evident in the research findings.
Although the level of body dissatisfaction among Lesbian, Bisexual, and Queer Women is not yet fully understood, research indicates that they may experience comparable or even higher levels of eating disorders compared to heterosexual women.
According to a systematic analysis conducted in 2022, the findings revealed that gay men exhibited a significant disparity between their self-perceived current and desired body fat, displayed a stronger drive for thinness, engaged in more body-related avoidance behaviors, were more inclined towards appearance fixing, experienced higher levels of overall body image disturbance, had a higher prevalence of eating disorder symptoms and body dysmorphic disorder pathology, and reported lower levels of body appreciation compared to heterosexual men.
Differences in eating disorder prevalence rates based on weight and body size:
Higher prevalence rates among individuals with lower weight and smaller body size:
According to a nationally representative sample, it has been found that over 30% of young adult females and over 15% of young adult males classified as overweight/obese reported having an eating disorder or engaging in disordered eating behaviors.
Having a larger body size increases the risk of developing an eating disorder and is often seen in individuals who experience bulimia and binge eating disorder. Interestingly according to research, people with larger bodies are only half as likely as those who are considered "normal weight" or "underweight" to receive a diagnosis of an eating disorder.
While the prevalent physical indicator of anorexia is typically characterized by insufficient body weight in relation to height, sex, and stature, it is crucial to acknowledge that an individual can still have anorexia without exhibiting low body weight.
Weight stigma and body dissatisfaction:
In the United States, research has shown consistent findings among overweight and obese adults. Both clinical and nonclinical samples have revealed that individuals who face weight-based stigmatization are more likely to engage in frequent binge eating, have a higher risk of developing maladaptive eating patterns and eating disorder symptoms, and have an increased likelihood of being diagnosed with binge eating disorder.
In line with similar research findings, studies have indicated that overweight and obese women who internalize negative weight stigma are more likely to report engaging in frequent binge eating and demonstrate a resistance to traditional dieting practices compared to overweight or obese adults who do not internalize stigma.
A study examining weight stigma and body dissatisfaction found that weight-based teasing and weight-related bullying were associated with increased body dissatisfaction and disordered eating behaviors.
Body image dissatisfaction across weight categories:
Body image dissatisfaction, which involves negative perceptions and feelings about one's own body, can contribute to the development of eating disorders.
In a study conducted with Italian university students, it was found that both men and women have a preference for thinness as an ideal body image. This emphasis on thinness, commonly observed in European countries such as Italy, Greece, and France, can contribute to the development of body image disturbance and subsequent feelings of dissatisfaction.
With a comprehensive understanding of the overall prevalence of eating disorders, it is crucial to delve deeper into the nuances of these rates across various demographics. By shifting our attention to the interplay of factors such as gender, age, socioeconomic status, and cultural influences, we can gain a more nuanced perspective on the prevalence rates of eating disorders.
The Dangerous Toll of Eating Disorders: Mortality Rates and Health Consequences
Eating disorders take a dangerous toll, causing severe health consequences such as physical complications, organ damage, and increased mortality rates. Shockingly, estimates reveal an annual loss of over 3.3 million healthy life years worldwide due to these disorders. This topic highlights the urgent need for intervention, treatment, and awareness to address the devastating impact of eating disorders on individuals' well-being.
Statistics on the mortality rates of individuals with eating disorders
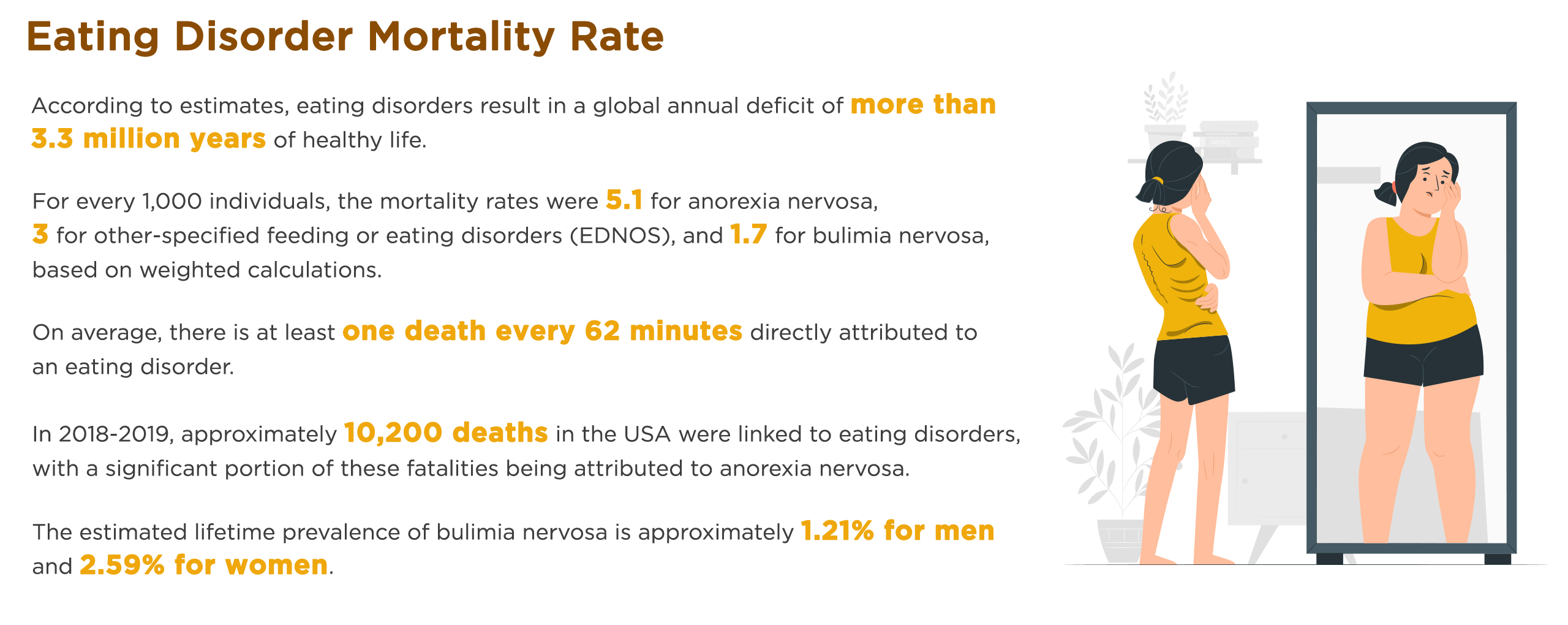
Anorexia nervosa:
Anorexia nervosa has the highest mortality rate of any psychiatric disorder, with a standardized mortality ratio of approximately 5.9.
In 2009, a longitudinal assessment of mortality over 8 to 25 years was conducted in 1,885 individuals with anorexia nervosa using computerized record linkage to the National Death Index. The study found a crude mortality rate of 4.0% for anorexia nervosa.
Research indicates that a concerning percentage of individuals with anorexia experience mortality rates within a specific timeframe. Approximately 10% of people with anorexia succumb to the illness within a decade of its onset, and this figure increases to 20% over a span of 20 years. Premature deaths in individuals with anorexia can be attributed to various factors, including cardiac complications, endocrine disorders, gastrointestinal diseases, refeeding syndrome, and even suicide.
Bulimia nervosa:
Individuals with bulimia nervosa have a higher risk of mortality than the general population, with a standardized mortality ratio of approximately 1.7.
Another study discovered that individuals diagnosed with bulimia nervosa had a crude mortality rate of 3.9%.
The most common causes of death in individuals with bulimia nervosa are medical complications related to purging behaviors, such as electrolyte imbalances and heart failure.
Binge eating disorder:
While individuals with binge eating disorder are not faced with immediate risks of mortality like those with anorexia or bulimia, there is a prolonged risk primarily associated with being overweight or obese. It is worth noting that two-thirds of individuals with BED are classified as obese, while many others fall into the overweight category.
However, individuals with binge eating disorder may be at increased risk of developing co-occurring health conditions, such as obesity and type 2 diabetes, which can increase the risk of mortality over time.
Other specified feeding or eating disorders (OSFED):
Research suggests that individuals with Other Specified Feeding or Eating Disorders face a notable risk of mortality, with crude mortality rates estimated at 5.2%. This indicates that a significant proportion of individuals diagnosed with OSFED experience death.
Untreated and persistent Other Specified Feeding or Eating Disorders can lead to various long-term complications, including gastrointestinal issues, weakened bones (osteoporosis), kidney damage, slowed growth, infertility, and heart conditions.
Confronting the Consequences: A Comprehensive Overview of Health Risks Associated with Eating Disorders
Heart problems - Eating disorders can cause a number of cardiovascular complications, including arrhythmia, low blood pressure, and heart failure. Among the patients included in the study, a total of 16 out of 45 individuals (36%) were found to have bradycardia. Further analysis revealed that of these 16 cases, 8 individuals were diagnosed with anorexia nervosa (AN), 5 individuals with bulimia nervosa, and 3 individuals with eating disorder not otherwise specified.
Gastrointestinal problems - Individuals with eating disorders may experience a range of gastrointestinal issues, including constipation, diarrhea, and gastroparesis (delayed emptying of the stomach). A well-known study conducted decades ago on 30 Anorexia Nervosa patients revealed a significant prevalence of esophageal motility disorders, including achalasia (23%) and other abnormalities (27%). According to a clinical review conducted in 2015, using the Rome II or Rome III criteria, it was found that 11-24% of patients diagnosed with eating disorders also met the criteria for functional constipation. The prevalence of constipation was particularly high among individuals with Anorexia Nervosa (AN), with reports ranging from 67% to 83% of AN patients experiencing constipation. Similarly, a significant proportion of patients with Bulimia Nervosa (BN), specifically 62.8%, also reported experiencing constipation.
Bone loss and osteoporosis - According to a study, eating disorders can lead to the development of osteoporosis or its precursor, osteopenia, which is characterized by reduced bone density. Specifically, it was found that approximately 90% of individuals with anorexia develop osteopenia, and 30% go on to develop osteoporosis. Moreover, having anorexia increases the risk of experiencing a bone fracture by at least three times.
Dental problems - Frequent vomiting, which is common in individuals with bulimia nervosa, can cause erosion of tooth enamel, cavities, and other dental problems. According to the American Dental Association, up to 89% of individuals with bulimia nervosa experience dental erosion.
Reproductive problems - Eating disorders can disrupt the menstrual cycle in women and lead to infertility. A study conducted in 2017 revealed the significant association between eating disorders and menstrual cycle disorders in girls. Among the participants, 236 girls (37.88%) were found to have irregular menstrual cycles, while 5.20% experienced secondary amenorrhea, which is the absence of menstruation.
Diabetes - Individuals with diabetes often exhibit disordered eating behaviors that can severely impact diabetes management. Additionally, diagnostic threshold eating disorders like anorexia nervosa, bulimia nervosa, and binge eating disorder may affect as much as 20% of individuals with diabetes. Specifically, it is estimated that up to 30% of individuals with type 1 diabetes experience an eating disorder, making eating disorders twice as prevalent in people with type 1 diabetes compared to those without the condition.
Obesity - In the realm of disordered eating, two conditions closely tied to overweight and obesity are binge-eating disorder (BED) and night-eating syndrome (NES). Those affected by BED face a notable connection to obesity, with estimates indicating that they are 3 to 6 times more likely to be obese compared to individuals without an eating disorder. Additionally, BED is associated with the onset of weight issues at an earlier age and a history of childhood obesity, with approximately 30% of those diagnosed with BED reporting struggles with obesity during their youth.
Death - Eating disorders have the highest mortality rate of any mental illness, research indicates that up to 10% of individuals with anorexia die within approximately 10 years of developing the illness, and up to 20% succumb to it within 20 years.
The Complexity of Eating Disorders: Exploring Risk Factors and Comorbidity
Having examined the prevalence rates of eating disorders across different demographics, we now turn our attention to understanding the complex nature of these disorders. In exploring the factors that contribute to their development and the coexistence of eating disorders with other mental health conditions, we gain a deeper understanding of the intricate dynamics involved.
Diving into the Causes: Overview of Risk Factors Associated with Eating Disorders
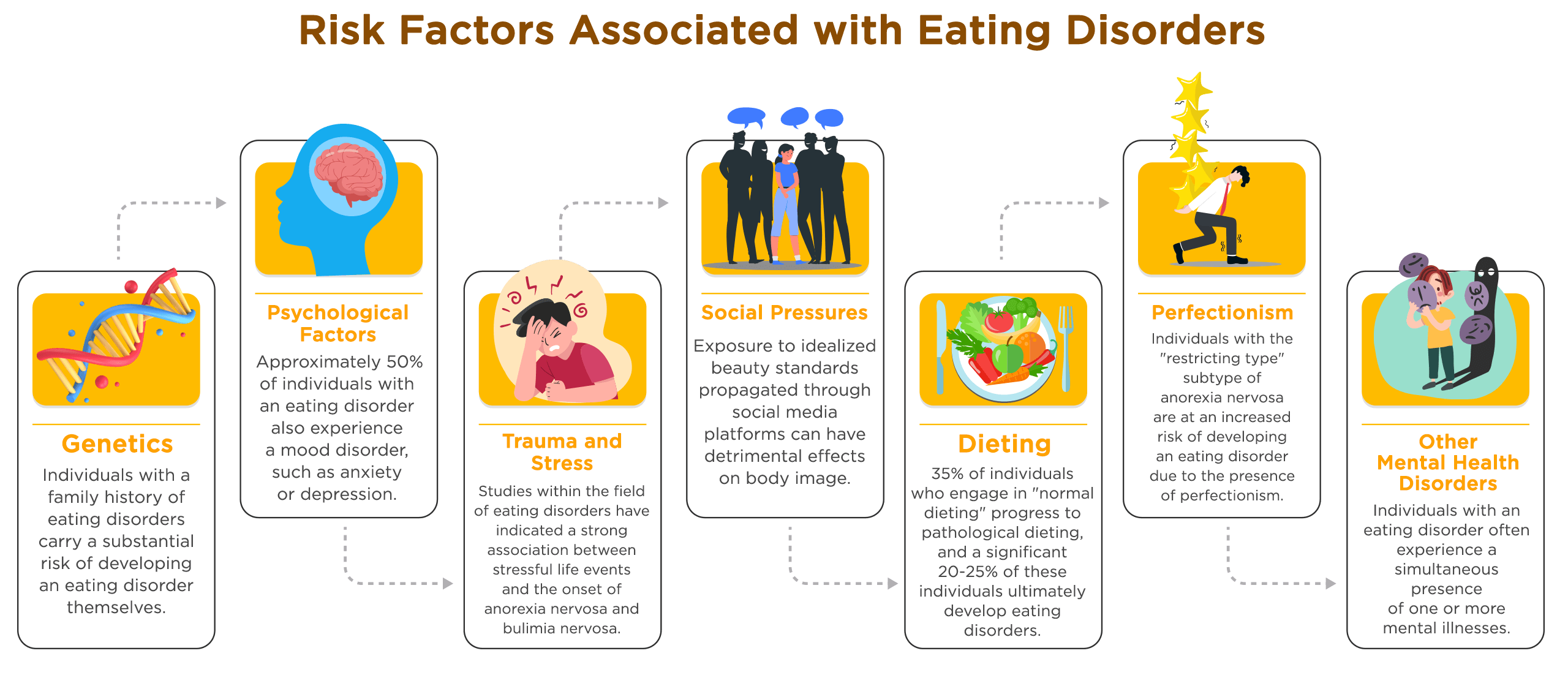
Genetics:
Individuals with a family history of eating disorders carry a substantial risk of developing an eating disorder themselves. Research has shown that having a close relative, such as a parent or sibling, with an eating disorder significantly increases an individual's susceptibility to developing similar disordered eating behaviors. In fact, individuals with a family history of eating disorders are up to 12 times more likely to experience an eating disorder compared to those without such a family history.
Research conducted on twins has provided valuable insights into the role of genetics in the development of eating disorders. Twin studies have demonstrated that genetic factors may contribute to approximately 50-60% of the risk for developing an eating disorder.
A study conducted in 2000 reported that approximately 58% of the risk for developing Anorexia nervosa can be attributed to genetic factors.
Psychological factors:
Co-occurring mental health disorders are frequently observed in individuals with eating disorders, highlighting the complex nature of these conditions. According to the National Association of Anorexia Nervosa and Associated Disorders, approximately 50% of individuals with an eating disorder also experience a mood disorder, such as anxiety or depression..
Individuals with eating disorders often have low self-esteem and report feeling a lack of control in their lives.
Trauma and stress:
Childhood abuse or trauma is a risk factor for developing an eating disorder later in life.
Numerous studies within the field of eating disorders have indicated a strong association between stressful life events and the onset of anorexia nervosa and bulimia nervosa. Specifically, in the case of adolescent anorexia nervosa, significant family conflict and disruption, changes in school or home environment, and heightened academic pressure have been identified as common stressful life events preceding the development of the disorder.
Social pressures:
According to the National Eating Disorders Association, a significant majority of teenage girls in the United States, accounting for 70%, acknowledge the influence of social media on their perception of the "ideal" body shape. Extensive research has demonstrated that exposure to idealized beauty standards propagated through social media platforms can have detrimental effects on body image, contributing to the development of negative body image, disordered eating behaviors, and heightened risks of experiencing depression and anxiety.
The pressure to conform to a certain body type can be particularly strong in certain subcultures, such as the fashion or fitness industries.
Dieting:
While dieting itself may not be the sole cause of eating disorders, it frequently serves as a precursor to their development. According to the National Eating Disorders Association, a notable 35% of individuals who engage in "normal dieting" progress to pathological dieting, and a significant 20-25% of these individuals ultimately develop eating disorders. The initiation of eating disorders is often linked to the adoption of restrictive diets, as they provide a means for individuals to exert control, meticulously track calories and fat content, restrict food types and quantities, and fixate on their weight.
Chronic yo-yo dieting (repeated cycles of weight loss and regain) is also a risk factor for developing an eating disorder.
Perfectionism:
Individuals with the "restricting type" subtype of anorexia nervosa are at an increased risk of developing an eating disorder due to the presence of perfectionism.
Studies have demonstrated that individuals diagnosed with anorexia nervosa and bulimia nervosa exhibit higher levels of perfectionism compared to individuals without eating disorders.
Other mental health disorders:
Research has uncovered a significant co-occurrence of eating disorders and substance use disorders, commonly known as a "dual diagnosis." In fact, a study revealed that approximately 27% of individuals with Anorexia Nervosa, 36.8% with Bulimia Nervosa, and 23.3% with Binge Eating Disorder (BED) also receive a diagnosis of a substance use disorder. Furthermore, the study highlights the undeniable relationship between substance use disorders and eating disorders, as 50% of those struggling with a substance use disorder also experience an eating disorder, in contrast to only 9% of the general population.
In a recent study conducted in 2021, it was revealed that Eating Disorders are intricate mental health conditions that frequently co-occur with other disorders. Individuals with an eating disorder often experience a simultaneous presence of one or more mental illnesses, including depression, anxiety, and obsessive-compulsive disorder (OCD).
The Intersection of Mental Health: Statistics on Comorbidity of Eating Disorders
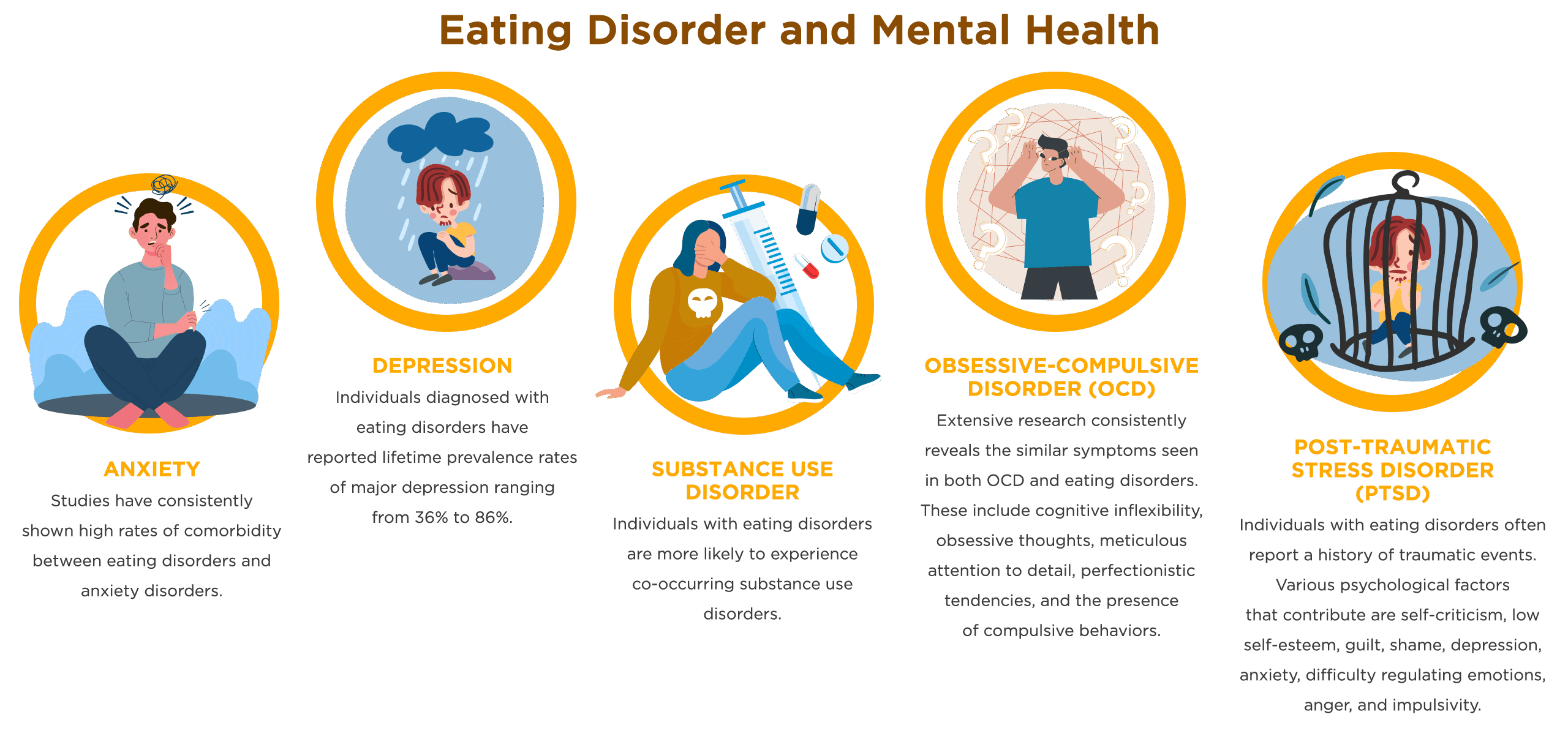
Anxiety:
Eating Disorders and Anxiety:
Studies have consistently shown high rates of comorbidity between eating disorders and anxiety disorders.
A systematic review and meta-analysis found that a significant proportion of women seeking treatment for an eating disorder also met criteria for comorbid anxiety disorders. Specifically, it was reported that approximately 65% of these women had at least one comorbid anxiety disorder. Furthermore, among those with comorbid anxiety disorders, around 69% reported that the onset of their anxiety disorder preceded the onset of their eating disorder.
Another study in individuals with anorexia nervosa, 83% of subjects and 71% of those with bulimia nervosa had been diagnosed with at least one anxiety disorder during their lifetime. The most common anxiety disorder among both anorexic individuals (55%) and bulimic individuals (59%) was social phobia. Importantly, in 75% of subjects with anorexia nervosa and 88% of subjects with bulimia nervosa, the comorbid anxiety disorder had emerged prior to the onset of the eating disorder.
Specific Anxiety Disorders and Eating Disorders:
There is evidence suggesting a hereditary component in both anorexia and anxiety disorders, which may be passed on to family members. In a study by Strober et al., it was observed that first-degree relatives of individuals with anorexia nervosa of the restricting type (including parents, siblings, and offspring who share approximately 50% of the same genes) have a threefold increased risk of developing generalized anxiety disorder (GAD).
A meta-analysis of 12 studies revealed the following rates of comorbidity between Eating Disorders and social anxiety:
Bulimia Nervosa: 84.5%
Binge Eating Disorder: 75%
Anorexia Nervosa (binge/purge subtype): 75%
Higher levels of social anxiety are associated with more severe Eating Disorder psychopathology and higher body weight.
The symptoms of Obsessive-Compulsive Disorder (OCD) and Eating Disorders (EDs) share similarities such as cognitive rigidity, obsessiveness, perfectionism, and compulsive behaviors. A meta-analysis examined the rates of comorbidity between OCD and EDs, revealing that the lifetime comorbidity rate was 18% and the current comorbidity rate was 15%. The prevalence of OCD was highest among individuals with Anorexia Nervosa, with a lifetime comorbidity rate of 19% and a current comorbidity rate of 14%. Follow-up data suggests that these comorbidity rates may double over longer periods of observation, reaching rates of 33%.
Depression:
Eating Disorders and Depression:
A significant proportion of individuals with eating disorders also experience comorbid Major Depressive Disorder (MDD), making it one of the most prevalent mental health diagnoses in this population. Studies indicate that approximately 50% to 75% of individuals with eating disorders also exhibit symptoms of depression. According to a study conducted in 2014, individuals diagnosed with eating disorders have reported lifetime prevalence rates of major depression ranging from 36% to 86%.
Recent research on eating disorders and depression has revealed a significant correlation between these two conditions. The statistics highlight the co-occurrence of major depressive disorder in individuals with specific eating disorders, such as anorexia nervosa, bulimia nervosa, and binge eating disorder. Here are the findings:
An estimated 32-39% of individuals with anorexia nervosa are diagnosed with major depressive disorder.
Approximately 36-50% of individuals with bulimia nervosa also have a diagnosis of major depressive disorder.
Among individuals with binge eating disorder, around 33% are diagnosed with major depressive disorder.
In a 2020 survey, the relationship between lifetime Major Depressive Disorder and the occurrence of Eating Disorders and disordered eating behaviors was explored, revealing notable findings.
13% met criteria for a lifetime Eating Disorder.
39% reported engaging in at least one lifetime clinically significant disordered eating behavior (e.g., binge eating) on the Structured Clinical Interview for DSM-IV.
In a large clinical database of women with EDs, 43% met criteria for a mood disorder, and 53% met criteria for an anxiety disorder.
In the National Comorbidity Survey Replication (NCS-R), over 80% of adults with lifetime bulimia nervosa had a lifetime anxiety disorder, and over 70% had a lifetime mood disorder.
A longitudinal study focused on adolescents, it was discovered that disordered eating behaviors and depressive symptoms tended to emerge simultaneously. More than half of the adolescent participants exhibited symptoms of a depressive disorder. The prevalence rates for Anorexia Nervosa and Bulimia Nervosa were comparable, with 51.5% and 54% of the sample, respectively, exhibiting these eating disorders.
In a 2015 study, which involved 271 patients diagnosed with eating disorders, it was found that 80% of individuals with anorexia nervosa (AN) had a prevalence of depression. Another study in 2004, which included 150 subjects (50 with restrictive Anorexia Nervosa, 50 with major depressive disorder, and 50 controls), reported a 36% prevalence of depressive symptoms in individuals with AN.
Shared risk factors and underlying mechanisms:
Eating disorders and depression share common risk factors and underlying mechanisms, including genetic, neurobiological, and environmental factors.
Based on the analysis using Akaike's information criterion values, the development of anorexia nervosa and major depression involves both genetic and unique environmental factors, with a genetic correlation between the two disorders of 0.58. The model suggests that approximately 34% of the genetic variance is shared between anorexia nervosa and major depression, with a confidence interval of 13% to 71%.
In 2022, studies exploring the relationship between eating disorders and trauma have predominantly focused on childhood sexual abuse. Notably, a significant minority of youth 40.9% have reported experiencing multiple instances of direct exposure to violence, abuse, or crime, emphasizing the importance of examining various types of trauma when investigating the association with eating disorders.
Substance use disorder:
Eating disorders and substance use disorder:
Eating disorders and substance use disorders have overlapping risk factors and underlying mechanisms, including genetic, neurobiological, and environmental factors. Extensive research has consistently demonstrated a strong association between these two conditions, with high rates of comorbidity observed. This indicates that individuals with eating disorders are more likely to experience co-occurring substance use disorders.
The co-occurrence of substance use disorders is a well-documented issue that complicates the treatment and outcomes of eating disorders. Notably, a recent meta-analysis revealed that 27.9% of individuals with eating disorders also had comorbid substance use disorders. Additional statistics on specific substance use disorders include:
Anorexia Nervosa: Lifetime prevalence of comorbid illicit drug use was 17.2%, and the prevalence of alcohol use disorder was 22.4%.
Bulimia Nervosa: Lifetime prevalence of comorbid illicit drug use was 18.6%, and the prevalence of alcohol use disorder was 24.0%.
It is important to highlight that alcohol, caffeine, and tobacco were among the most commonly reported substances associated with these comorbidities.
Data from the National College Health Assessment survey conducted by the American College Health Association between fall 2015 and spring 2019 were utilized for this study. The following statistics were found regarding substance misuse among students with eating disorder indications:
Prevalence of Substance Misuse among Students with Eating Disorder Indications:
Students with eating disorders were 7.43 times more likely to be diagnosed with Substance Use Disorders than peers without eating disorder indications.
1.91 times more likely to misuse cigarettes
1.81 times more likely to misuse e-cigarettes
1.16 times more likely to misuse alcohol
1.69 times more likely to misuse marijuana
2.91 times more likely to misuse cocaine or methamphetamine
3.42 times more likely to misuse sedatives
3.26 times more likely to misuse hallucinogens
8.35 times more likely to misuse opiates
6.36 times more likely to misuse inhalants
3.65 times more likely to misuse MDMA
10.37 times more likely to misuse other club drugs
2.09 times more likely to misuse prescription painkillers
2.43 times more likely to misuse prescription sedatives
2.03 times more likely to misuse prescription stimulants
Obsessive-Compulsive Disorder (OCD):
Eating disorders and obsessive-compulsive disorder (OCD):
Extensive research in the field has consistently highlighted the shared symptomatology between Obsessive-Compulsive Disorder (OCD) and eating disorders. This includes common features such as cognitive rigidity, obsessive thoughts, excessive attention to details, perfectionistic tendencies, and the presence of compulsive behaviors.
A systematic review conducted in 2022 aimed to provide a clearer understanding of the comorbidity rates between these conditions.
Lifetime comorbidity rate: The systematic review revealed that 18% of individuals with eating disorders also had a lifetime diagnosis of obsessive-compulsive disorder.
Current comorbidity rate: The study found that 15% of individuals with eating disorders had a concurrent diagnosis of obsessive-compulsive disorder at the time of data collection.
Long-term observation: The authors noted that over longer periods of observation, the prevalence of comorbidity may increase, with some follow-up data indicating comorbidity rates as high as 33%.
Anorexia Nervosa: Prevalence rates of obsessive-compulsive disorder were found to be highest among individuals with Anorexia Nervosa, with a lifetime comorbidity rate of 19% and a current comorbidity rate of 14%, compared to other subtypes of eating disorders.
In 2020, extensive research focused on the coexistence of obsessive-compulsive disorder (OCD) and eating disorders, revealing valuable insights into their prevalence and interconnectedness on a global scale. These findings shed light on the intricate relationship between OCD and eating disorders, highlighting the varying rates of comorbidity depending on the specific type of eating disorder and the temporal perspective under consideration.
Lifetime comorbidity rate: Among patients with EDs, the worldwide prevalence of lifetime comorbidity with OCD was found to be 18%.
Current comorbidity rate: The concurrent presence of OCD and EDs was observed in approximately 15% of patients during the study period.
Anorexia Nervosa: In the case of anorexia, the lifetime comorbidity rate with OCD was slightly higher at 19%, while the current comorbidity rate was 14%.
Bulimia Nervosa: Rates of comorbid OCD were slightly lower in bulimia nervosa, with a lifetime comorbidity rate of 13% and a current comorbidity rate of 9%.
Significance of current comorbidity: The current presence of OCD was significantly more frequent in anorexia compared to bulimia.
Prospective follow-up studies: Long-term investigations yielded higher estimates of lifetime comorbidity, with overall EDs at 38%, anorexia at 44%, and bulimia at 19%.
Bidirectional relationship between eating disorders and OCD:
The interplay between eating disorders and obsessive-compulsive disorder (OCD) is multifaceted and reciprocal, with both conditions mutually influencing and intensifying each other. There exists a significant overlap between eating disorders and OCD, potentially indicating shared neurobiological, genetic, or psychological factors. Although earlier descriptive studies reported high rates of obsessional or compulsive features in eating disorder patients ranging from 50% to 100%, more recent research has revealed a lower prevalence of such features.
In a recent study, researchers discovered that the co-occurrence of Anorexia Nervosa and obsessive-compulsive disorder (OCD) is notable. Here are the key findings:
19% of individuals with Anorexia Nervosa developed OCD during their lifetime.
14% of participants already had a comorbid diagnosis of Anorexia Nervosa and OCD.
Obsessive-compulsive behaviors were observed in a significant proportion of patients with anorexia nervosa, ranging from 35% to 44%.
2015 findings support the presence of shared genetic influences between obsessive-compulsive disorder (OCD) and anorexia nervosa (AN), indicating a potential genetic overlap. However, it is important to note that each disorder also has distinct genetic and environmental risk factors contributing to its development. The twin analyses revealed the following results:
Obsessive-compulsive disorder (OCD):
Approximately 66% of the variation in OCD can be attributed to genetic factors.
Around 34% of the variation is influenced by environmental factors.
Anorexia nervosa (AN):
Roughly 38% of the variation in AN can be attributed to genetic factors.
Approximately 62% of the variation is influenced by environmental factors.
The correlation between the genetic factors of OCD and AN was found to be 0.52, indicating a moderate positive relationship. Additionally, the unique environmental factors showed a correlation of 0.11, suggesting a weak positive relationship. These results indicate that while there are shared genetic influences between OCD and AN, there are also unique environmental factors that contribute to each disorder independently.
Post-Traumatic Stress Disorder (PTSD):
Eating disorders and post-traumatic stress disorder (PTSD):
The association between eating disorders and traumatic experiences, including symptoms of post-traumatic stress disorder (PTSD), is widely recognized. Individuals with eating disorders often report a history of traumatic events, and a review of the literature identified several psychological factors that contribute to this association, including self-criticism, low self-worth, guilt, shame, depression, anxiety, emotion dysregulation, anger, and impulsivity. The prevalence rates of PTSD among different eating disorders vary, as follows:
Anorexia Nervosa: Prevalence rates of PTSD range between 16.1% and 22.7%.
Bulimia Nervosa: Prevalence rates of PTSD range between 32.4% and 66.2%.
Binge Eating Disorder: Prevalence rates of PTSD range between 24.02% and 31.6%.
Research has consistently shown a significant association between eating disorders and PTSD, with high rates of comorbidity.
A study conducted in 2015 examined the prevalence of post-traumatic stress disorder (PTSD) among 103 individuals with eating disorders, with an average age of 29.1 years. The participants completed standardized questionnaires to assess their PTSD status. The findings revealed the following:
The overall prevalence of PTSD among the sample was 24.3%.
Among individuals with anorexia nervosa (AN), 23.1% met the diagnostic criteria for PTSD according to the DSM-IV.
Among individuals with bulimia nervosa (BN), 25.5% met the diagnostic criteria for PTSD.
A significant majority of patients (67.7%) reported experiencing their first traumatic event prior to the onset of their eating disorder.
Bidirectional relationship between eating disorders and PTSD:
The relationship between post-traumatic stress disorder (PTSD) and eating disorders is complex and bidirectional. Studies have indicated that individuals with anorexia nervosa are more likely to develop PTSD over time, and conversely, those with PTSD have a higher likelihood of developing anorexia nervosa. In the context of residential treatment for eating disorders, it has been found that around 75% of women report a history of trauma, with 50% of them having a diagnosis of PTSD. Additionally, a strong correlation has been observed between binge eating behaviors and PTSD.
According to a 2021 study, there is a significant overlap between Binge Eating Disorder (BED) and Post-Traumatic Stress Disorder (PTSD). The research revealed that approximately 26% of women diagnosed with BED also met the criteria for PTSD. Both disorders share common features, including negative mood states, low self-worth, and difficulties in regulating emotions. Individuals who have experienced trauma may turn to binge eating as a maladaptive coping mechanism, providing temporary relief and triggering brain responses associated with euphoria. Additionally, those with BED and PTSD often experience challenges in impulse control.
The Bottomline
In this article, we delve into the critical aspects of eating disorders, including their prevalence rates, comorbidity with mental health conditions, health consequences, and underlying risk factors. These disorders have a significant global impact, affecting diverse populations with varying rates. By actively pursuing knowledge and disseminating information, individuals can recognize signs, intervene early, and provide support for individuals affected by eating disorders, fostering a more empathetic and informed society. To drive change and support to those affected by eating disorders, it's important to educate yourself and others, spreading awareness and understanding. Challenge societal stigmas and promote empathy. Advocate for improved access to treatment and support services.

Licensed Marriage & Family Therapist
7 years of practice
I love being a therapist. I'll help you get clarity on your situation and provide you with tools that you can carry with you for life.
Recommended Articles


